Featured Science
Till two or three decades ago, the commonest causes of death in India were communicable diseases like typhoid, cholera, malaria, dengue and tuberculosis. Over the last 20 – 30 years, this situation has undergone a dramatic change in India. Slowly, but steadily, the incidence of communicable diseases started declining. This was replaced by a rapid rise in non-communicable diseases (NCDs) which includes diabetes, hypertension, obesity, cardiovascular diseases, stroke and cancer. According to the Global Burden of Diseases India Study, in 1991, only Kerala state had more than 50% of deaths due to NCDs in the whole of India. By 2016, in all 31 states and union territories of India, NCDs constituted more than 50% of all deaths, and in some states like Kerala and Tamil Nadu, almost 75% of all deaths were due to NCDs.
Among all NCDs, diabetes is one of the most easily measured disorders. Indeed, by looking at the prevalence rates of diabetes, one can predict the prevalence of non-communicable diseases in the country. In the early 1970s, an Indian Council of Medical Research (ICMR) study showed that about 2% of individuals in urban areas and about 1% individuals in rural areas in India had diabetes. At that time, diabetes was considered mainly a migrant Indian disorder because already Indians living abroad in countries like US, UK, South Africa, Fiji and Mauritius had double digit rates of diabetes which was much higher even compared to the local host population whether they were Whites, Blacks, Chinese or other ethnic groups.
In 1991, the opening up of India’s economy took place, and with this, the socio-economic situation in India changed rapidly. People started becoming more affluent, and this brought it in its wake a rapid rise in obesity rates in India. This was primarily due to the consumption of energy dense foods which were rich in carbohydrate, fat and calories. This led, not only to a rapid increase in diabetes, but also to increase in obesity and hypertension and to some extent, increases in cancer rates as well.
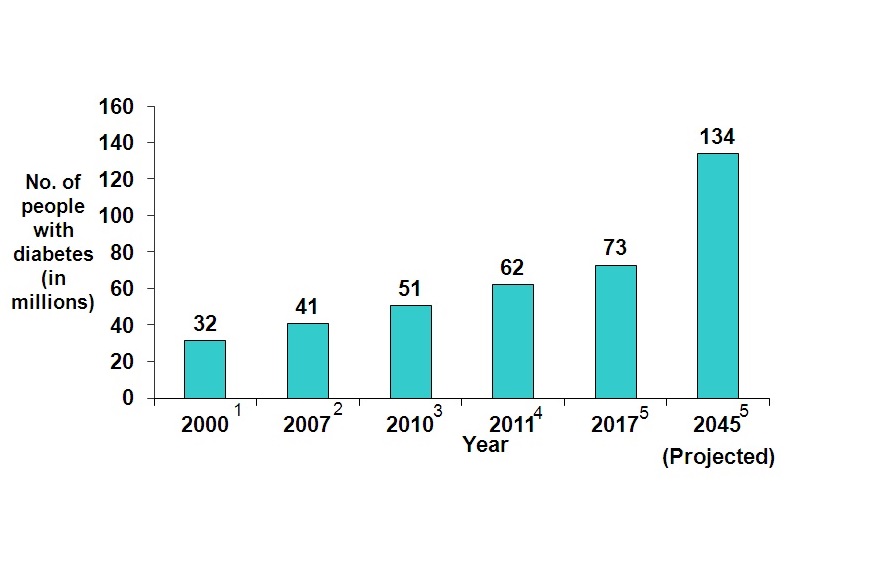
Recent studies have shown that in cities like Chennai and Delhi, the prevalence of diabetes is now almost 22 – 24% of the adult population aged 20 years and above. By age 55, in these cities, almost 40% have diabetes and an additional 35% have pre-diabetes! In rural areas, especially in some states like Bihar and Jharkhand, diabetes rates are still relatively low. However, in the more developed southern states, the prevalence of diabetes even in rural areas, has risen very sharply and now varies from 14–18%. Indeed, in some states like Kerala, the rural prevalence of diabetes may actually be higher than in urban areas. The total number of people with diabetes in India was 32 million in the year 2000. This increased to 41 million in 2007 and further increased to 62 million in 2011, and in 2017 to 73 million people. This is further expected to increase in 134 million people by the year 2045, as depicted in figure
What is the cause of the rapid rise in diabetes in India?
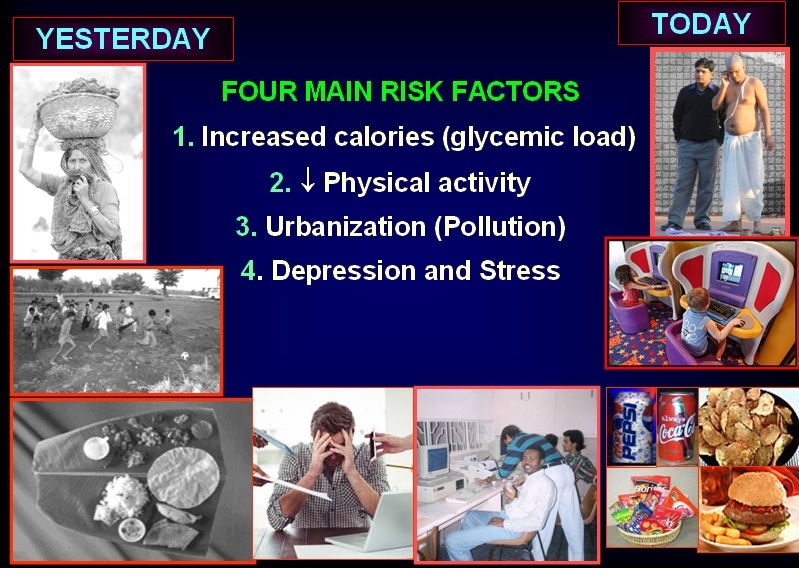
The main drivers of the diabetes epidemic are 1) Change to unhealthy diets leading to increased calories and glycemic load 2) Reduction in physical activity 3) Urbanization (Pollution) & 4) Depression and stress as depicted in the figure.
Why is there epidemic of diabetes in India?
Dietary changes
Traditionally, the diets in India up to the 1960s or 1970s consisted of whole cereals which were made of complex carbohydrate and had higher fibre. In the south and eastern parts of India, mainly unpolished or hand pound rice (brown rice) was mainly consumed by people, while in the north and west, it was whole grain or unpolished wheat. Due to rapid developments in milling technologies, the rice became polished more and more and eventually was completely depleted of its bran or the outer covering and what was left was only the pure endosperm or starch. Similar changes occurred with wheat consumption in the west and north India. Today, consuming white rice is almost like consuming, like glucose.
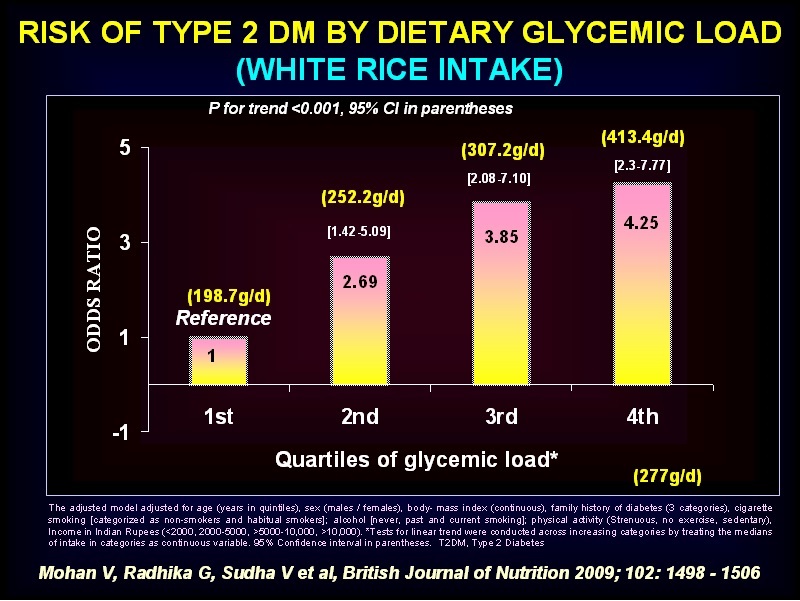
This Figure below shows that when Rice consumption goes up from about 200 to 400 gms/day, the risk for diabetes rises four fold.
With the increasing affordability of people, more and more consumption of not only rice but also oil, sugar, and fat occurred. People started eating out more frequently in hotels and restaurants which meant that they were eating foods that were higher in these unhealthy food items. At the same time, an influx of western diets occurred with pizzas, burgers and soft drinks loaded with sugar, all becoming fashionable. The calorie, carbohydrate, and sugar & fat contents of the diets increased sharply. This resulted in insulin resistance and eventually to the pancreas being unable to cope with the demand for insulin leading to beta cell exhaustion and thus to diabetes.
Decline physical activity levels
Side by side, along with the rapid changes in diet, there was also a rapid decline in physical activity. Thanks to improved socio-economic status, people started using motorized transport in the form of two wheelers and four wheelers. Villagers who used to walk miles to go somewhere now had better transport facilities. Farmers, who used to till the soil and plough the fields manually, could now sit on tractors and get their work done. Escalators and elevators became fashionable and people stopped using stairs, even when available. Thus the physical activity of people declined rapidly.
outside food became more common. This deadly combination of unhealthy diet coupled with physical inactivity completely changed the health scenario of the country. This means that the energy expenditure is much less than the energy intake. It is therefore hardly surprising that disorders which were normally seen only in middle age, like obesity, diabetes and hypertension started occurring in young adults and soon in adolescents and children.
Newer risk factors for diabetes
Along with an unhealthy diet and physical activity, stress and depression increased. This was partly due to long working hours and because youngsters now started working to US timings in call centres, in the IT industry, etc, which meant that their normal sleep patterns were affected. Newer etiologies for diabetes meanwhile were uncovered. Pollution (both outdoor and indoor), use of pesticides, adulteration of foods and the use of bisphenol components (due to the use of plastics), which act as endocrine disruptors, have all been shown to be directly or indirectly linked to the occurrence of diabetes.
What can be done to stem the epidemic of diabetes?
The good news is that prevention of diabetes is possible. As diabetes is an asymptomatic disease, one has to start screening early, particularly in high-risk groups. The Indian Diabetes Risk Score (IDRS) [Table 1], developed by us shows who is at the risk of diabetes. If the risk score is more than 60, then one is at high risk of diabetes.
Table 1 : Indian Diabetes Risk Score (IDRS)
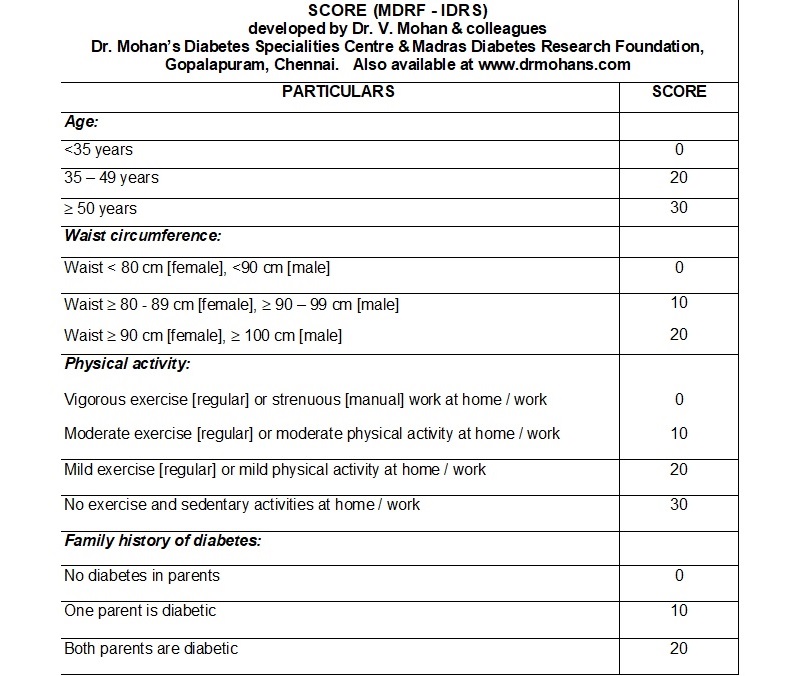
If the score is….
³ 60: Very HIGH RISK of having diabetes. Oral Glucose Tolerance test is recommended to rule out diabetes. If this is not possible, at least a Random Blood sugar or a Fasting Blood Sugar should be done
30 – 50 : The risk of having diabetes is MODERATE . It is still recommended to have the above check up.
<30 : Risk of having diabetes is probably LOW
Note : The Indian Diabetes Risk Score applies only to common type of diabetes called as Type 2 Diabetes. People with Type 1 and other forms of diabetes need not have high risk score
By adopting a healthy lifestyle by cutting down on carbohydrates and calories and adding sufficient protein in the form of vegetable proteins like Bengal gram, green gram, black gram, mushroom, soya, milk or egg white and including healthy fats like monounsaturated fat which includes nuts, seeds, groundnut oil, mustard oil, etc, the diet can be made more healthy. Consumption of plenty of green leafy vegetables and fruits also constitutes a healthy diet.
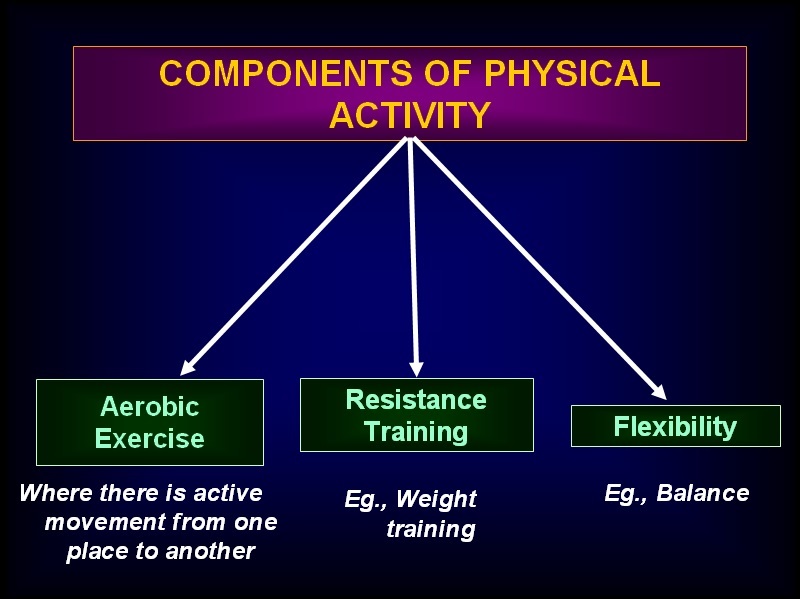
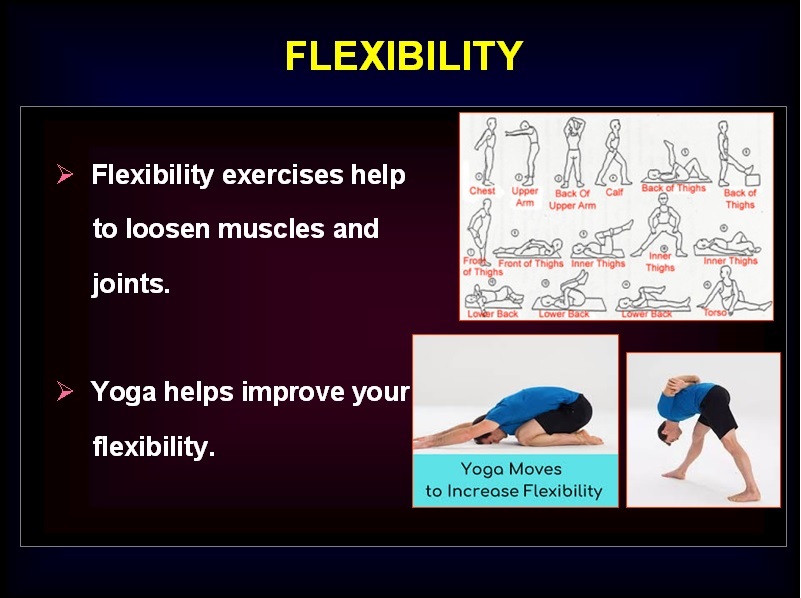
In addition, physical activity must be encouraged. The recommendation is to have at least 30 mins of exercise, eg, a brisk walk, at least 5 times a day amounting to a minimum of 150 mins/week. There are 3 components of physical activity: Aerobic exercise, Resistance training and Flexibility as shown in the Figure below :
Stress reduction in the form of yoga, meditation and relaxation is also helpful to prevent diabetes. Finally, one should avoid pollution and adulteration of foods as this can also help to reduce the incidence of diabetes.
Today, there are more people with pre-diabetes than diabetes in the country. This presents a window of opportunity to prevent diabetes because we can start early in the natural history, we can reverse diabetes. Studies at our centre have shown that it is possible to prevent diabetes in up to 35% of people with pre-diabetes, by just adopting simple lifestyle measures like diet, exercise and some weight reduction. If these messages of healthy lifestyle are introduced in the community, we can prevent several million people from developing diabetes. If this is not done, in the years to come, millions of young adults with diabetes would run the risk of not only developing diabetes but also heart attacks, losing their limbs due to gangrene, going blind or developing renal failure needing dialysis or renal transplantation. All these are not only expensive, but also affect the quality of life of the individual, the family and the society. On a macro level, this can affect the very economy of the country itself, because it can lead to absenteeism and loss of productivity. There is therefore, an urgent need for individuals, the family, the society and communities as well as government and non-governmental organizations to work together to stem the tide of the diabetes epidemic.

THE TIME TO ACT IS NOW!
DR. V. MOHAN,
Chairman & Chief of Diabetology,
Dr. Mohan’s Diabetes Specialities Centre & Madras Diabetes Research Foundation
References
1. Wild S et al, Diabetes Care, 2004; 27: 1047 – 1053
2. Diabetes Atlas, International Diabetes Federation, December 2006
3. IDF Diabetes Atlas, 4th Edition, International Diabetes Federation, 2009
4. Anjana RM, Mohan V, et al for the ICMR – INDIAB Study group, Diabetologia. Dec 2011; 54: 3022 – 3027
5. IDF Diabetes Atlas, 8th Edition, 2017